Clinical Networks have been providing evidence-based service improvement in the NHS since 9th February 1999.
With over 20 years of service improvement, Clinical Networks are still delivering clinical change in the UK in 2020. Our journey can be traced back to 1999 when managed clinical networks were introduced within the NHS in Scotland [1].
Managed Clinical Networks were first set up in the UK
In 2000, the then Labour government introduced a 10-year modernisation programme for the NHS. Clinical Networks were seen as performing a crucial role in the delivery of that programme.
The NHS Plan was published:
a 10-year modernisation programme of investment and reform.

In 2002 researchers identified that network organisations had several theoretical advantages in terms of their flexibility, robustness, and ability to respond quickly to a rapidly changing environment[2].
Networks offered a way of making the best use of scarce specialist clinical expertise, standardising care, improving access, and reducing any “distance-decay” effects that can result from the concentration of specialist services in large centres. They could create systems to ensure that all patients received a standard investigation regardless of whether they lived near a specialist centre or not and were referred on rather than being held in a local service which might not have the full range of expertise. This appeared to have been an important reason for the growth of networks in cancer and coronary heart disease.
The cancer networks started to report significant benefits as a result of being able to focus on the needs of their patients without the distraction of managing the less patient focused parts of the system such as non-clinical support services. In critical care, networks had been used to increase efficiency and responsiveness by combining scarce resources to iron out the effect of variations in demand.
A real attraction of networks was identified as a focus on clinical issues to create organic and flexible organisations that can respond well to a changing environment[3].
The existing regional health authorities were renamed and merged to form 28 new Strategic Health Authorities, under the National Health Service Reform and Health Care Professions Act 2002. This was the first time that the regional tier in the NHS reported directly to the centre rather than having a board and non-executive members.
Many Clinical Networks in the UK were now hosted by Strategic Health Authorities.
The importance of professionals working in managed or structured networks transferring knowledge to spread innovation, was highlighted again in 2005 research[4]. In 2005, Sir Nigel Crisp accelerated the adoption of practice-based commissioning, bringing commissioning decisions closer to GPs and patients.
The Government accelerated the timetable for the introduction of practice-based commissioning through the publication of the report: Commissioning a patient-led NHS

By 2007, Clinical Networks were facing some challenges. Researchers found that the initial knowledge-sharing purpose of the cancer clinical networks had undergone top-down ‘distortion’ by the demands of the Labour government’s focus on organizational restructuring and adhering to government targets. This resulted in a superficial bottom-up adoption of the networks model and limited impact upon organizational processes[5].
In 2007, there was a change of government and the Conservative’s vision for the future of the NHS was published.
The Conservative Party outlined its vision for the future of the NHS in the White Paper:
Lord Darzi had been asked to work with the Strategic Health Authorities throughout the country to adopt similar recommendations to those in his 2007 report Healthcare for London: A framework for action, a major review into the future of London’s health services, throughout the country.

The Conservative Party outlined its vision for the future of the NHS in the White Paper:
NHS autonomy and accountability: Proposals for legislation
In 2009, Strategic Health Authorities reviewed their workload, against the new legislation and the recommendations of the ‘next stage review’.
As a result of this review, South Central SHA and South East SHA wound up the Mental Health, Older Persons, Maternity and Children’s clinical networks. They were replaced by Darzi workstreams. The Central South Coast cancer clinical network continued but was now hosted by Portsmouth Hospitals with a staff of ~20 WTE. The cardiovascular clinical network was a similar size and staff were transferred to the management of Hampshire Primary Care Trust (PCT).
Strategic Health Authorities across the country start to implement the ‘NHS next stage review’ and Health Minister, Lord Darzi, leads what becomes known as outlines his 10-year vision for the NHS in the report, High quality care for all.

In 2010, network forms were found by researchers to be particularly effective in tackling ‘wicked problems’ or problematic social situations where: (1) there is no obvious solution; (2) many individuals and organizations are necessarily involved; (3) there is disagreement among stakeholders; and (4) where desired behaviour changes are part of the solution. So-called ‘wicked’ problems go beyond the scope of one agency (for example, anti-crime or smoking strategies) and the term applies where unaligned interventions by one agency have perverse side effects. Instead, in order to solve these problems, a broad systemic response is required, working across boundaries and engaging citizens and stakeholders in co-producing, policymaking and implementation[6].
[6] https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1467-9299.2010.01896.x

A 2012 study into clinical networks in Australia reinforced the net benefits that can be achieved by this approach[7].
Following the implementation of the Health and Social Care Act in 2012, the NHS Commissioning Board (which would later become NHS England) was created and the cancer and cardiovascular clinical networks were brought back under the management of the local area office (Wessex). A mental health, neurology and dementia network was set up. The clinical networks were renamed as ‘Strategic Clinical Networks’ with the aim of focusing on domains and transformational projects (with different areas taking a lead on different projects) based on the model in Alberta, Canada. The cancer and cardiovascular network workforce was spread over the five new networks.
The outcomes had been very promising in Alberta for cardiovascular services: Early results showed reductions in average length of hospital stay by half, improved access to rehabilitation, and better stroke outcomes. This work won the coveted cochairs award at the 2014 Canadian Stroke Congress for most innovative patient care programme. The Alberta Mental Health Clinical Network reduced inappropriate antipsychotic use by 20% and the Alberta Surgery Clinical Network extended compliance to the safe surgery checklist from 47% to 94%[8].
[7] https://link.springer.com/article/10.1186/1748-5908-7-108
The rationale behind the re-establishment of clinical networks based on the Alberta model was because in 2012 most years of life were still being lost in the UK from Cancer, Mental Health and Cardiovascular Services rather than other conditions and it was recognised that the greatest difference in health outcomes could still be achieved by improving health of mothers/fathers and health in the first five years of life (Maternity/Children).

NHS reorganisation: The Coalition sponsored Health and Social Care Bill 2010/11 proposed significant reforms to increase the influence of GPs on commissioning, increase competition and abolish strategic health authorities (SHAs) and primary care trusts (PCTs). Following nearly 18 months and thousands of amendments, the Health and Social Care Bill was passed in 2012.
In 2014, the Health Foundation reviewed a diverse range of networks rather than focusing on one type. Even where no formal network structure existed, the researchers found network benefits could be created and felt, so networks that evolve informally can also have an important role in quality improvement.
Successful networks had a clear direction, credibility, scale and reach. They enhance knowledge and encourage innovation while creating meaningful relationships. Networks could focus energy and momentum directly and exclusively on quality improvement, unlike many other types of organisation. They could provide a neutral environment where people from different organisations, disciplines and constituencies – including patients and service users – could connect and collaborate on an equal footing.
Finally, it became apparent how highly members valued networks because of indirect effects such as enhancing social connectedness or reducing personal risk. The Health Foundation found that effective networks have five core features that add value to quality improvement[9]: Critical mass, community building, co-operation, collective intelligence and structure.
NHS England publishes its Five-Year Forward View.
The NHS South Region of NHSE was established.
[9] https://www.health.org.uk/sites/default/files/EffectiveNetworksForImprovement.pdf
The 5C Wheel
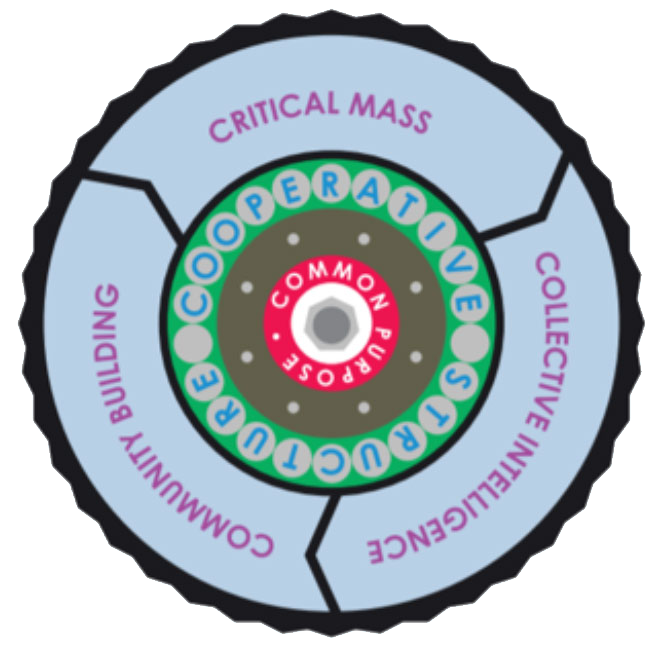
Health Foundation conducts and in-depth review of networks and finds that effective networks have five core features in common.

In 2015, following the publication of the Five-Year Forward View, the focus of the Wessex, Thames Valley and Kent Surrey Sussex Managed Clinical Networks was changed by NHS England. The Cardiovascular network concentrated on the Diabetes Prevention Programme and the work of the Maternity Clinical Network (everywhere but Wessex) was picked up by the Nursing Directorate.
In 2016, a systematic review found that successful networks were those that had adequate resources, credible leadership and efficient management, coupled with effective communication strategies and collaborative, trusting relationships. The importance of well-designed and strategically aligned projects, and effective partnerships with operational leaders (i.e., front-line health services delivery teams), professional organizations and with academic institutions (whose researchers lead or contribute to network projects)[10].
NHS Improvement launches (Dido Harding was appointed Chair in 2017).
Sustainability and Transformation Plans were first published.

In 2018, researchers found that the presence of established formal or informal Clinical Networks supported the development of CCG clinical leadership and resulted in improvements in patient pathways. There was some concern that this may have been a mitigation against the fragmentation of services in 2012 rather than a substantial shift in patient benefit. The three arenas identified where clinical networks made a difference supporting CCGs were:
- Policy making, Budget holding, Commissioning strategy (setting this at CCG Board)
- Operational Commissioning
- Practice Delivery[11].
In 2018 we celebrated the 70th anniversary of the NHS, and Thames Valley Strategic Clinical Network produced this summary of their achievements to date.

In 2019, there was the publication of the NHS Long Term Plan and a joint working programme began to bring together staff in NHSE and NHSI under one management structure.
From 1st April 2020, in order to bring the Cancer Alliances closer to the specialist cancer NHS Trusts in the region, the Wessex Cancer Alliance was to be chaired by a specialist cancer NHS Trust Chief Executive (from University Hospital, Southampton), the Thames Valley Cancer Alliance was to be chaired by Oxford NHS Trust. The Kent and Medway Cancer Alliance was chaired by a specialist provider (yet to be determined) and the Surrey and Sussex Cancer Alliance was to be chaired by Royal Surrey County NHS Trust. The line of managerial accountability and the level of resource for the four Cancer Alliances is now very different to that of the Clinical Networks.
The staff in the three Clinical Networks in the South East (Wessex, Thames Valley and Kent Surrey Sussex) became part of two Clinical Delivery and Network teams: Hampshire Thames Valley and Kent Surrey Sussex. The Kent Surrey and Sussex Clinical Network footprint remained the same. Both teams were now jointly responsible for supporting STPs/ICSs in the delivery of Long-Term Plan priorities across South East of England.
Publication of the NHS Long Term Plan. The NHS Long Term Plan set out the aim that every part of England would be covered by an integrated care system by 2021, replacing STPs but building on their good work to date.
NHS England and NHS Improvement Joint Working Programme established
Organisational NHSE/NHSI restructuring into two regions in the South – South East and South West
2020 – further adaptability and flexibility was required from the Clinical Delivery and Network Teams as staff were redeployed to the COVID response, creating vacancies and new priorities. The Hampshire and Thames Valley and Kent Surrey Sussex Clinical Delivery and Network teams started to work together across the South East supporting systems and STPs/ICSs in the new cell structure from March. Our work in mental health, palliative and end of life care and maternity continues.

With thanks to The Nuffield Trust – from whom some of the timeline is borrowed:
https://www.nuffieldtrust.org.uk/health-and-social-care-explained/nhs-reform-timeline/